KNOWLEDGE HUB

If you are sitting up late at night, staring at a genetic test report that mentions a de novo mutation, you are likely feeling a heavy mix of relief and fear. You might finally have a name for your child’s challenges, but that name comes with a new set of questions that feel urgent and overwhelming. Parents often find themselves asking: "Did I pass this on?" or "What does this mean for my other children?".
This guide is here to walk you through those questions with clarity. While this information is educational and not a replacement for the personalized advice of your genetic counselor, it will help you understand the biology behind these results and how they affect your family’s future.
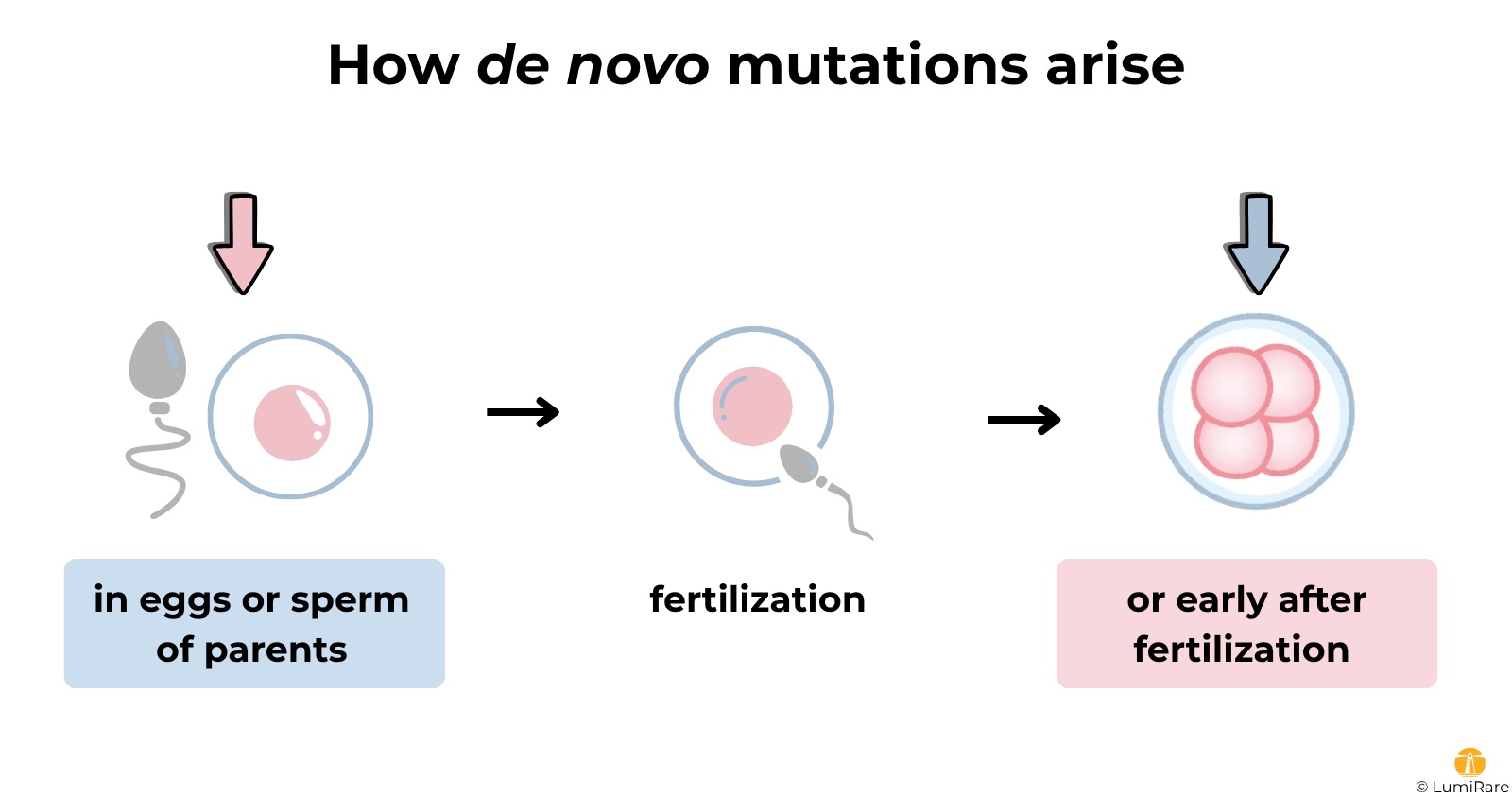
The term de novo is Latin for "new". In the world of genetics, a de novo mutation (or variant) is a genetic change that is present in the child but is not found in either parent’s DNA. When a lab labels a variant this way, they are saying that when they tested the mother and the father, the specific change seen in the child was simply not there.
To understand how this happens, think of the human genome as a massive library of instructions. Most of the time, we inherit our "books" directly from our parents. However, a de novo mutation is like a brand-new typo that appears in the child’s version of the book; a typo that wasn't in the parents' copies.
In almost every case, this "typo" occurs in one of two ways. It either happens in the specific egg or sperm cell that formed the child, or it occurs very early after fertilization during the first few cell divisions of the embryo. It is a random event that occurs naturally in human reproduction.
One of the most important things for a parent to hear is this: A de novo change is not "caused" by anything you did during pregnancy. It is not the result of what you ate, the stress you felt, or any lifestyle choices you made.
These changes are a fundamental part of being human. Every person is born with a small handful of de novo mutations; most of them are harmless and never noticed. It is only when one of these random "typos" happens to land in a critical gene, such as one responsible for brain development or heart function, that it leads to a medical condition. When a child has significant symptoms but there is no family history of the disorder, a de novo variant is often the most likely explanation.
To be sure a variant is de novo, the lab usually needs to perform trio testing. This means they sequence the DNA of the child and both biological parents at the same time. By comparing the three results directly, the lab can see that the child carries the variant while the parents do not.
Sometimes, a child is tested first on their own. If the lab finds a suspicious variant, they will then recommend "targeted testing" for the parents to see if they carry it. If the parents test negative for that specific variant, the lab can then classify it as de novo.
However, there are technical limits to these tests. For example, a parent might carry the variant at such a low level in their blood that it falls below the "detection limit" of the machine. There are also rare biological reasons, like mosaicism, which we will explore below, that can make these results slightly more complex than a simple "yes" or "no".
Seeing de novo on a report is a powerful clue, but it doesn’t automatically mean the variant is the cause of your child’s condition. To decide if a variant is truly "disease-causing," clinicians look at the phenotype match, which is a fancy way of asking: "Does this gene actually control the parts of the body where the child is struggling?".
If the gene is known to cause developmental delays or epilepsy, and your child has those symptoms, the de novo status becomes strong evidence for a diagnosis. Doctors also look at the "disease mechanism". Some genes cause problems if they are "turned off" (loss-of-function), while others cause issues if they are "too active" (gain-of-function). A de novo variant is most convincing when the type of "typo" matches how that specific gene is known to break down.
If the variant is labeled as a VUS (Variant of Uncertain Significance), the de novo status is a "lead" that may point toward an answer, but it is not yet a confirmed diagnosis.
The question of whether this could happen in a future pregnancy is often the most pressing concern for families. In general, if a variant is truly de novo and neither parent has it in their blood, the risk of it happening again is considered low.
However, genetics is rarely 100% certain. This is where the concept of mosaicism becomes important.
You might wonder: "If my DNA blood test was negative, how could the mutation happen again?" The answer lies in where the mutation lives. Somatic mosaicism means a parent has the variant in some of their body's cells (like skin or blood) but not others.
Germline (or gonadal) mosaicism is more hidden. This means a parent carries the mutation in a portion of their reproductive cells (eggs or sperm). Because standard genetic tests usually use blood samples, they cannot "see" what is happening in the egg or sperm cells.
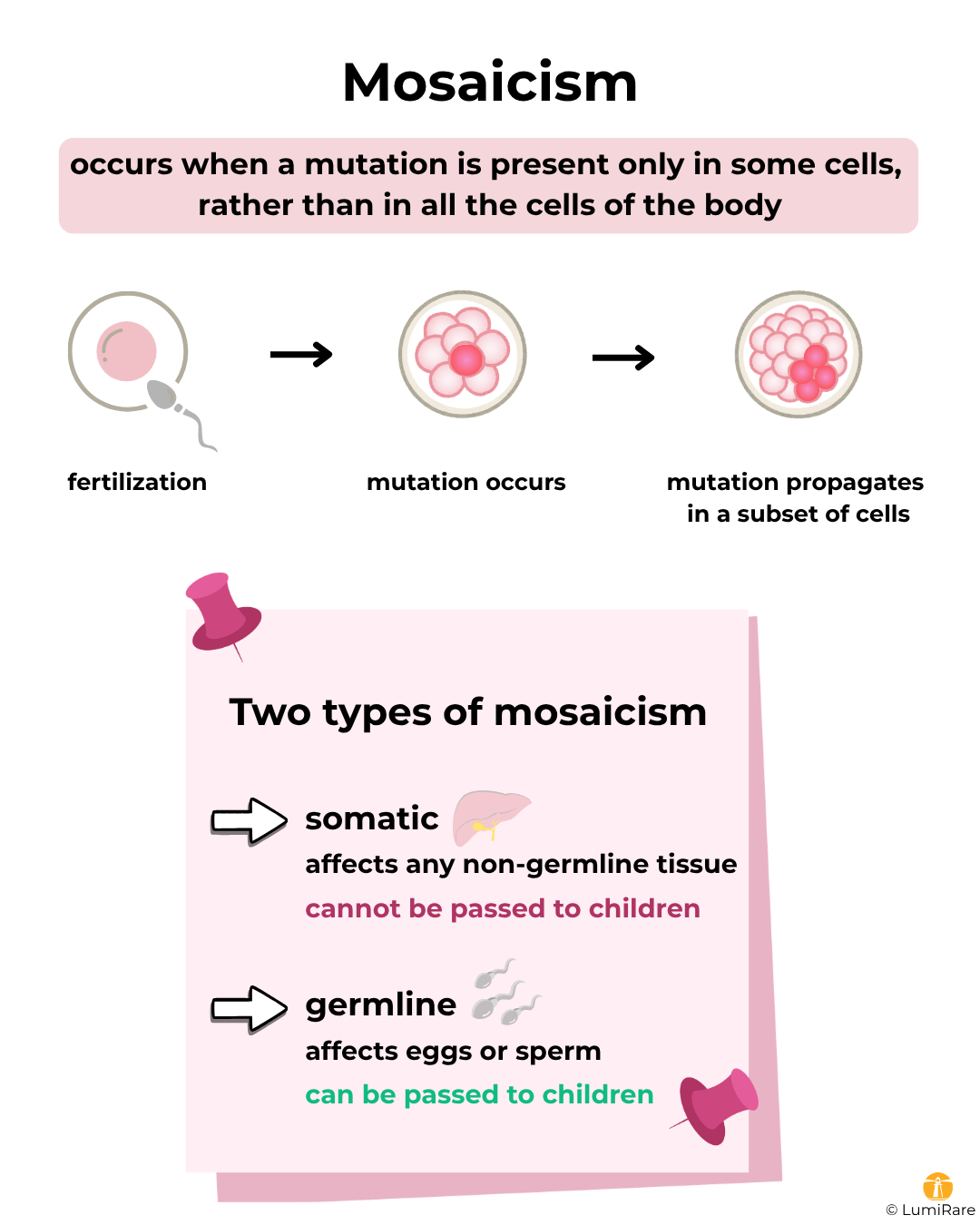
If a parent has germline mosaicism, there is a small but real chance the same variant could appear again in a future child. This is why clinicians typically discuss recurrence risk in ranges rather than a single "yes" or "no". It is not something you can control; it is a biological reality that genetic counselors take into account when helping you plan for the future.
If a variant is confirmed as truly de novo and the parents' blood tests are negative, the child's siblings are usually very unlikely to carry the same variant. De novo mutations typically do not raise concerns for extended relatives like aunts, uncles, or cousins.
There are exceptions, of course. If a sibling shows similar symptoms, or if there is a suspicion of parental mosaicism, a doctor might recommend testing the siblings just to be sure. Most of the time, however, the "new" nature of the mutation means it started with your child and is not something running through the rest of the family tree.
Moving Forward: Questions for Your Geneticist
When you go to your next appointment, it can be helpful to have a structured list of questions to ensure you get the most out of your time with the specialist. You might consider asking:
Summary
Finding a de novo mutation is often the first step toward understanding your child’s unique journey. Remember these core facts:
López-López L, Lapeña-Gil L, Benítez Y, Serrano C, Sánchez-Barbero AI, Blanco-Kelly F, et al. Accurate and cost-effective workflow integrating trio pooled-WES for novel gene discovery in neurodevelopmental disorders. Eur J Hum Genet. 2026. doi:10.1038/s41431-026-02075-0.
Mohiuddin M, Kooy RF, Pearson CE. De novo mutations, genetic mosaicism and human disease. Front Genet. 2022;13:983668. doi:10.3389/fgene.2022.983668.
This text was written by the LumiRare team – researchers specialising in rare diseases.
This content is for educational purposes only; it does not constitute medical advice.
Would you like to find out what science has to say about your genetic finding?
LumiRare’s researchers analyse scientific articles and highlight what may be most relevant to your situation.
FOLLOW FOR RARE DISEASE
RESEARCH UPDATES